
Female Genital Tissue
- teachanatomy

- Apr 13
- 16 min read
The female reproductive system, also known as the female genital system, is a group of organs and structures that work together to enable pregnancy, and childbirth. Its specific functions include:
Production of the female gametes, the ova.
Production of female sex Hormones (estrogen and progesterone).
Facilitate fertilization of the ovum by spermatozoa.
Transport of the fertilized ovum to the uterus.
Facilitate implantation of the blastocyst.
Formation of the placenta and maintenance of the unborn child during the entire period of gestation
Birth of the child and expulsion of the placenta
Production of milk to feed the newborn.
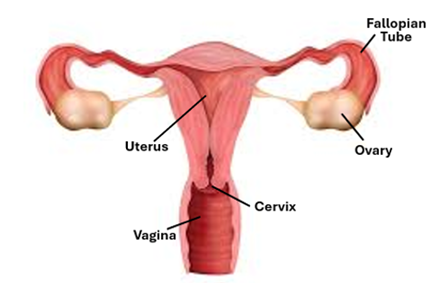
The system consists of:
Ovaries
Fallopian tubes
Uterus
Cervix
Vagina
External genitalia
The mammary gland
Ovary
The ovaries, right and left are the female gonads that produce the female gametes. Each is an oval-shaped structure, about 6cm long in reproductive women; they diminish in size after menopause. The ovary consists of an inner medulla, surrounded by an outer cortex and invested by a connective tissue capsule, which is covered by mesothelium (germinal epithelium). The hilum, a shallow surface depression, is the site of entrance of blood vessels and nerves into the ovary. Embryologically, the ovary is of mesodermal origin; it develops from the gonadial ridge of the mesoderm. The ovarian capsule is a dense irregular connective covered a single layer of cuboidal mesothelial cells that constitute a germinal epithelium. Beneath the capsule is the tunica albuginea, which is a thin condensed connective tissue layer. The cortex has supportive stroma made of stromal cells and follicles. When normally functioning, it is characterized by the presence of different types of ovarian follicles, which include primordial follicles, primary follicles, secondary follicles, tertiary follicles and mature Graafian follicles, in addition to degenerate atretic follicles and corpora lutea.
The medulla is formed of a loose connective tissue rich in blood vessels and nerves that enter the medulla via the ovarian hilum. The medullary blood vessels include spiral arteries known as the helicine arteries. Branches emerge from these vessels and supply the cortex. The ovarian activities are modulated by the pituitary follicle stimulating hormone (FSH) and luteinizing hormone (LH).

Follicular Development
At birth a baby girl’s ovarian cortex contains a large number of primordial follicles (about 500. 000). Each primordial follicle consists of a primary oocyte and a single layer of flat follicular cells surrounding the oocyte. At the onset of puberty, the pituitary gland starts release FSH, which stimulates development of the primordial follicles to develop. The release of FSH is periodical and the development of the primordial follicle is also periodical. Each month, under the influence of FSH a cohort of about 20 primordial follicle are recruited for development. They enlarge mainly due to enlargement of the follicular cells changing their shape from flat cells in cuboidal cells or low columnar cells, Then the follicular cells become FSH-dependent and more responsive to FSH, and start to proliferate forming two, three or more layers of follicular cells around the primary oocyte, instead of the single layer of flat cells. In this way the recruited primordial follicles develop into primary and then secondary follicles. A follicle with a single layer of cuboidal follicular cells is called a primary follicle, whereas a follicle with more than one layer of granulosa cells is called a secondary follicle. Concurrently, the primary oocyte enlarges and a clear homogenous eosinophilic membrane called the zona pellucida appears around the primary oocyte separating it from the surrounding follicular cells. Still under the influence of FSH, the follicular cells start to secrete estrogens and fluid containing estrogen starts to build around the follicular cells. Eventually, fluid-filled vesicles appear in-between the follicular cells. When the fluid-filled spaces appear between the follicular cells, the ovarian follicle is referred to as tertiary follicle or early antral follicles.

Preantral and Antral Follicles
A preantral follicle is a follicle where a theca layer present. The theca layers develops from the stromal cell that surround the growing follicle. The stroma cells start to arrange themselves encircling the developing follicle delineating it from the surrounding stroma. The process commences in the secondary follicle stage and gets more and more evident as the follicles develops becoming more prominent in tertiary follicles. Thus, a tertiary follicle is a preantral follicle consisting of primary oocyte surrounded a clear zona pellucida, follicular cells containing fluis filled space and clear stromal cell investment known as the theca folliculi.

The fluid filed cavities of tertiary follicles coalesce to form a single large cavity called the antrum; the follicle then becomes known as a antral follicle. It continues to enlarge; when it reaches a diameter of 0.5mm it is called a Graafian follicle. This is the follicle that releases the oocyte at the time of ovulation. The fluid contained within the antrum is called the follicular fluid or the liquor folliculi. The mature Graafian follicle is a well differentiated structure. It is characterized by a large clearly defined antrum full of liquor folliculi. The follicular cells surrounding antrum constitute the stratum granulosum. The layer follicular cells that immediately surround the oocyte elongate, become columnar and appear as if they are radiating from the oocyte; this single layer of radiating follicular cells constitute the corona radiata. A prominent homogenous eosinophilic zona pellucida separates the oocyte and the corona cells. The accumulation of cells that anchor the oocyte and the corona cells to the rest of follicular cells is called the Cumulus oophorous. A well-developed theca folliculi invests the whole follicle. It has two layers; a more cellular theca interna and a more fibrous tunica externa. Theca interna cells are endocrine cells that produce an steroid called androstenedione. Granulosa cells take up androstenedione and transform it to estrogen. Granulosa cells also produce small amounts of follicular FSH and inhibin. A thick basement membrane separates theca interna from the stratum granulosum; this is known as the glassy membrane. Theca interna cells are cuboidal or thick ovoid cells. In addition to androstenedione, they produce small amounts of progesterone. The theca externa cells are spindle-shaped cells similar to stromal cells; they have contractile abilities, and by their contraction they may help in the process bursting of the follicle and release of the oocyte at the time of ovulation. The oocyte of Graafian follicle completes the first meiotic division become a secondary oocyte after releasing a polar body, the first polar body.

Ovulation and Corpus Luteum
Of the several primordial follicles that are recruited for developing as a cohort under the influence of FSH, only one follicle ovulates; the rest of the follicles undergo apoptosis at various stages of follicular development. Prior to rupture of the mature Graafian during ovulation, the primary oocyte completes its first meiotic division, releases a polar and develops into a secondary oocyte. Thus, the oocyte which is released from the ovary at the time of ovulation is secondary oocyte. Under the influence of the pituitary LH, granulosa and theca interna cells of the ruptured Graafian follicle transform into pigment containing and progesterone producing endocrine cells known as luteal cells. These luteal cells are of two types, large granulosa luteal cells and smaller theca luteal cells that develop from the stratum granulosum and the theca interna respectively. They both produce progesterone and smaller amounts of estrogen. At the early stages of the formation of the corpus luteum blood from ruptured vessels fill the former antrum. Such a structure is called the corpus hemorrhagicum. If fertilization takes place the corpus luteum persists as a corpus luteum of pregnancy, otherwise it is a cyclic corpus luteum that will regress by the end of the menstrual period.

Atretic Follicles and Corpora albicans
Follicles that do not reach maturity and ovulation undergo apoptosis, which is a programmed cell death, to form atretic follicles. Atretic follicles are made degenerating cells and often show a thickened glassy membrane When the corpus luteum regresses, particularly the corpus luteum of pregnancy it leave a prominent scar known as the corpus albicans

Mesothelium and Ovarian interstitium
A single layer of cuboidal epithelial cells covers the ovarian surface. It is the mesothelium, which has also been known as the germinal epithelium. The mesothelium rests on a thin basement membrane that separates it from the tunica albuginea, which is a layer of dense connective tissue. The ovarian stroma or interstitium is compact, rich in cells and poor in fibers. Stromal cells are spindle shaped and have the potentiality of developing into theca cells; theca interna cells are steroid secreting endocrine cells.
Oogenesis
This is the process whereby ova are formed. It begins during fetal period and is completed only at the time of fertilization. It is essentially similar to spermatocytogenesis, i.e. mitosis followed by meiosis. There is no cell shape transformation as in spermiogenesis, instead the cell grows greatly into a huge cell known as the oocyte or egg cell. Oogenesis is characterized by two arrests of meiosis, one in the prophase of the first meiotic division and the other in metaphase of the second meiotic division.
Oogenesis commences during fetal period where oogonia divide by mitosis and give rise to primary oocytes. Primary oocytes go into meiosis-1 but this is arrested in the prophase of the first meiotic division; it takes place during diplotene of meiosis-1 when the homologous chromosomes separate from each other. Meiosis-1 remains arrested for years and is not completes until the primary oocyte is about to be released from the ovary during ovulation. The end result od meiosis-1 are two cells genetically identical, but morphologically quite dissimilar, a huge cell called the secondary oocyte and a minute cell called the first polar body. The secondary oocyte is released during ovulation and immediately goes into the 2nd meiotic division without DNA replication, meiosis-2 is also arrested; it is arrested in the metaphase and is not completed until a sperm head penetrate the oolemma during fertilization. Meiosis-2 also yield daughter cells identical genetically both being haploid, but morphologically dissimilar; one is huge and called the ovum and the other is tiny and called the second polar body.

Fallopian Tube
The fallopian tube, also known as the uterine tube and oviduct, is an 10cm long channel for transportation of the ovum from the ovary to the uterus. It is the site of fertilization where sperms meet the ovum and fertilize it. It is a tubular organ that has four parts, infundibulum, ampulla and isthmus. The infundibulum is the widened funnel-shaped initial part closest to the ovary that covers the ovary with its finger-like projections. Ampulla is middle part where fertilization usually takes pales whereas the isthmus is the part connected to the uterus. The wall of the Fallopian tube wall consists of three mucosa tunica, the mucosa, muscularis and serosa. The mucosa consists of a epithelium and a lamina propria. The epithelium is mostly simple columnar epithelium but has basal cells in some regions and thus appears pseudostratified. It contains three types of cells; these are the columnar ciliated cells, the secretory and intercalated cells. The ciliated cells are more numerous in the distal parts of the Fallopian tube, in the infundibulum and neighboring parts of ampulla. By the rhythmic movements of their cilia, they help in transport of the ovum towards the uterus. The secretory cells are tall columnar non-ciliated cells that are more active in secretion during ovulation; they are more numerous in the proximal parts of the ampulla and the isthmus. Their secretion constitutes a vehicle for transport of the ovum and movement of the sperms. It also provides nutrients for the fertilized ovum. The intercalated cells, also known as peg cells, are probably secretory cells depleted of their secretory granules. The lamina propria of the fallopian tube is highly cellular; it contains numerous spindle-shaped cells along with fibroblasts and thin collagen fibers. It does not contain glands but shows branching folds that are particularly prominent and complicated in the ampulla. The tunica muscularis become progressively thicker towards the uterus. It comprises a well-developed inner circular layer and a thinner outer longitudinal layer; both made of smooth muscle fibers. Their contractions produce peristaltic movements that assist in the transport of the ovum towards the uterus.

The Uterus
The uterus is a hollow pear-shaped organ where embryo implantation and fetal development take place. It is a hormone-response female reproductive organ. The uterus has a thick wall that consists of an endometrium, myometrium and epimetrium. The endometrium is tunica mucosae of the organ, the myometrium is its tunica muscularis, and the perimetrium is the serosa. The endometrium consists of an epithelium which is a simple columnar epithelium, and the lamina propria which is a highly cellular loose connective tissue. It contains the simple tubular uterine glands that undergoes cyclic changes in response to hormones in adult fertile women. The myometrium is made of 3-4 layers of smooth muscle fibers, whereas the epimetrium (perimetrium) is a typical serosa. It is lacking in the caudal parts where it is replaced by am adventitia.
Endometrium
The endometrium is the uterine mucosa consisting of an epithelium and a lamina propria. The epithelium is simple columnar; few cells may be ciliated. The lamina propria is highly cellular; it contains many spindle shaped (decidual) cells that secrete small amounts of prostaglandins and fibrinolysin. It contains simple tubular uterine glands; their basal ends could be branching. The endometrium has two layers: an upper functional layer and a deep basal layer. The functional layer can be divided into a superficial compact zone and a deeper spongy zone (layer). The functional layer is lost (sloughed off during menstruation). The basal layer remains unaffected by the cycle

Endometrial Cycle
The endometrium undergoes cyclic changes during the monstrous cycle under the influence of female sex hormones i.e. estrogen and progesterone. During menses, the functional layer (the stratum functionalis) is lost. During the ovarian follicular phase and under the influence of estrogen, the endometrium proliferates and regenerates from the basal layer (the stratum basalis); this endometrial phase is known as the proliferative phase. During the ovarian luteal phase and under the influence of progesterone, the uterine glands become tortuous and highly secretory; this endometrial phase is known as the secretory phase.

Endometrial gland development occurs under the influence of estrogen that causes endometrial gland proliferation in order to lay the foundation for the subsequent receptive, secretory phase when pregnancy will be established. The proliferating glands show mitotic figures that indicate cell division, multiplication and spreading. The glandular epithelium may appear pseudostratified, the lumen undiluted and stroma highly cellular.
The secretory phase follows the proliferative phase and is the phase where uterine gland secretions rich in nutrients are released into the uterine lumen to nourish the incoming fertilized ovum or the embryo before implantation. The uterine glands become highly coiled taking as corkscrew appearance at this phase; the coiling greatly increases the glandular cell surface area available for secretion. The lumina of glands become wider as more and more secretion passes from the secretory cells into the lumen. The gland secrete glycogen, accordingly the secretory cells contain large amounts of glycogen , particularly in their basal parts. Glycogen is water soluble and is washed out during routine histological preparations, therefore the glandular secretory cells at this phase appear pale or foamy. This phase is maintained by high progesterone levels.

Endometrial Cycle and Blood Vessels
The basal layer of the endometrium is supplied by straight short arteries whereas the functional layer is supplied by spiral helicine arteries. Decline in ovarian hormones causes constriction of the helicine arteries leading ischemia of the functional layer and its sloughing off resulting menses.

The Cervix
The uterine cervix is the lower narrow end of the uterus that connects the uterus to the vagina; it is a muscular, tunnel-like organ about 2-3cm long. The cervical wall consists of a mucosa made up of an epithelium and the lamina propria and the muscularis which is made of smooth muscle fiber, surrounded by an adventitia.
The cervix has two parts: the endocervix (cervical canal) and ectocervix, the endocervix and the external os. The endocervix which is also known as the cervical canal, is lined by simple columnar epithelium, whereas the external os, which is also known as ectocervix is lined by stratified squamous epithelium.
Lamina propria is collagenous connective tissue. The surface epithelium invaginates into the lamina propria in the form of furrows or clefts that appear in histological sections as if they are simple tubular glands. The epithelial cells are secretory cells that produce mucus. The activity of these glands and consistency of their secretion are influenced by the ovarian sex hormones.
The Vagina
The vaginal wall is made of a mucosa, muscularis and adventitia. The mucosa has folds known as rugae and is lined by a stratified squamous nonkeratinized epithelium. The lamina propria rich in elastic fibers and is devoid of glands. The muscularis is made of smooth muscle and the outermost layer is the adventitia which made of a collagenous connective tissue.

The Breast
The breasts or the mammary glands are highly modified apocrine sweat glands which develop embryologically from the ectoderm, the future epidermis. The breasts of both sexes develop similarly from birth to puberty. At puberty the female breasts enlarge under the influence of pituitary and ovarian hormones which cause epithelial proliferation and increased adipose tissue deposition. The breast of adult women undergo cyclical changes under the influence ovarian hormones until menopause. After menopause, the breasts undergo progressive atrophy and involutional change. The primary function of the female mammary gland is production of milk for nourishment of the newborn.
Each breast consists of 15 to 25 independent units called breast lobes, each lobe containing a compound tubulo-alveolar gland. The size of the lobes is variable and each of the larger lobes lobe connects to the surface via a duct, the lobar duct. Before opening onto the surface, each of these duct forms a dilatation called the lactiferous sinus. Smaller lobes have in blind-ended ducts that do not reach the nipple surface.
The adipose component of the mammary gland forms a large portion of the breast’s fat pad. The variation in breast size amongst women is related to the adipose tissue volume rather than the epithelial component itself. Adipose tissue is abundant in the interlobular spaces and scarce within lobules. Breast lobes are embedded in a mass of adipose tissue, subdivided by collagenous septa. The adipose tissue actively participates in mammary gland homeostasis and milk production.
The breast stroma consists of a loos connective tissue made of a ground substance, fibers and cells. The ground substance contains proteoglycans, hyaluronic acid and fibronectin, whereas the fibers are type-1 and type-3 collagen fibers. Fibroblasts are the commonest type of cells, and they are the source of the ground substance and fibers.
The nipple contains bands of smooth muscle, oriented parallel to the lactiferous ducts and circularly near the base. Contraction of these muscle bands causes erection of the nipple. The nipple contains orifices of the lactiferous ducts. These orifices have tiny sphincters that prevent leakage during breastfeeding. A circular, pigmented skin known as the areola surrounds the nipple. Areolar skin is subject to darkening during puberty, pregnancy, and sexual arousal and orgasm. The peripheral regions of the areola contain several nodular elevations known as tubercles of Morgagni, which contain the openings of Montgomery glands. These glands are modified glands that represent an intermediate stage between sweat and true mammary glands. They secrete a substance that provides lubrication during breastfeeding.
Within each lobe of the breast, the lobar duct branches repeatedly to form a number of terminal ducts, each of which leads to a lobule consisting of multiple alveoli. Each terminal duct and its associated lobule are called a terminal duct–lobular unit. The lobules are separated by moderately dense collagenous interlobular tissue, whereas the intralobular supporting tissue surrounding the ducts within each lobule is less dense and more vascular.
The breast ducts and acini are lined by two layers of cells, a luminal layer of epithelial cells and a basal layer of flattened myoepithelial cells. In the larger ducts, the luminal epithelial cells are tall columnar cells. whereas, in the smaller ducts and acini the epithelial cells are cuboidal. A layer of myoepithelial cells surrounds the ductal epithelial cells. The epithelium of the lactiferous sinuses is similar to that of ducts of the breast; close to the surface the epithelium transforms into a stratified squamous epithelium. The interlobular ducts are surrounded by dense fibrous interlobular connective tissue and adipose tissue.

Breast during pregnancy
Changes that take place in the mammary glands during pregnancy are attributed to the lactogenic hormones pituitary gland, the placenta and the ovaries, namely prolactin, human chorionic somatomammotropin, estrogen and progesterone. Under the influence of these hormones the duct epithelium proliferates to form more ducts and secretory acini. The breast lobules increase in size at the interlobular connective tissue. The lining epithelial cells vary from cuboidal to low columnar. As pregnancy progresses, the acini begin to secrete a protein-rich fluid called colostrum, the accumulation of which causes dilation of the acinar lumen. As compared to milk, colostrum contains little lipid.
Lactating breast
After parturition, progesterone levels decrease, lifting its inhibitory effect over prolactin, and prolactin stimulates copious milk secretion in conjunction with oxytocin. The lactating breast is composed almost entirely of acini distended with milk, and the interlobular tissue is reduced to thin interlobular septa. The acini appear under the microscope filled with an acidophilic substance with vacuoles; milk proteins stain acidophilic and the vacuole are lipid droplet that dissolved during tissue processing. The epithelial cells are flattened and the acini distended by secretions. A neurohormonal reflex, initiated by suckling, causes the release of the hormone oxytocin from the pituitary. Oxytocin causes contraction of the myoepithelial cells which surround the secretory acini and ducts, thus squeezing milk out of the lobules into the lactiferous sinuses; this is known as milk-let-down. After weaning, withdrawal of the suckling stimulus, and the associated release of pituitary hormones causes regression of the lactating breast and resumption of the normal ovarian cycle.


Comments